
In a new paper just published online in Maternal & Child Nutrition, we use survey data to tackle some basic myths about milk sharing in the U.S.: Who are people sharing with? What kinds of information is being gathered? How is milk being shared?
Below are key points of the paper, broken down myth-buster style:

5 MYTHS OF MILK SHARING
MYTH 1: MILK SHARING IS BUYING & SELLING HUMAN MILK
There is all kinds of confusion about whether milk selling is the same as milk sharing, and whether differences between the two matter in terms of the potential risks.
We asked survey respondents with milk sharing experience if they had ever bought or sold milk in addition to milk sharing. Here’s what they reported:
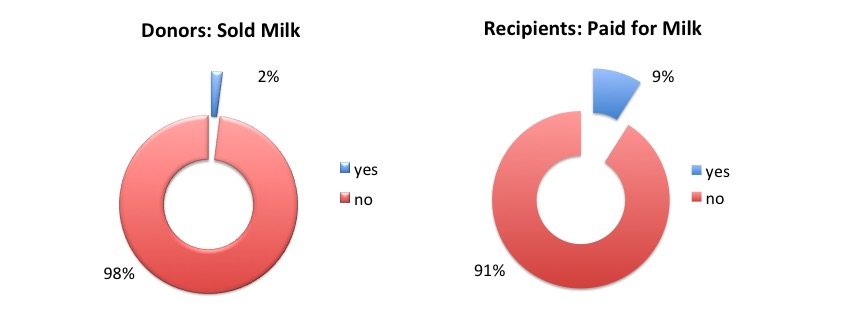
These findings are consistent with other reports of milk sharing practices. While a small number of respondents did both milk buying/selling and milk sharing, the evidence suggests that milk sharing is a gift economy. In other words, milk sharing IS NOT the same thing as milk selling.
MYTH 2: MILK SHARING IS CASUAL
You may have heard people refer to milk sharing as “casual” milk sharing. This term is loaded with stigmatizing assumptions, not the least of which is that milk sharing operates similarly to online dating, a practice that may lead to casual, even anonymous, sexual encounters. Calling milk sharing “casual” also implies that it is being done blindly, without regard to the risks.
Sooo…..is milk sharing casual?
- Of 867 respondents, there were no cases of anonymous milk sharing.
- 29% shared ONLY with family members or friends.
- Everyone who had received shipped milk asked donors screening questions and/or shared only with friends and family members.
- In cases where milk was either bought or sold, recipients reported asking screening questions, meeting donors in person, and/or buying milk from a milk bank.
Does this mean milk sharing is never anonymous? Not necessarily. But, our findings are consistent with other studies that describe milk sharing as being practiced by people who, if they aren’t already family or friends, become well-acquainted as part of milk sharing interactions.

MYTH 3: PARENTS ARE SEEKING MILK FOR SICK BABIES
For some time now, people have been trying to understand the dynamics between milk banking and milk sharing. Many have argued that the people who engage in milk sharing, both as donors and recipients, are doing so in response to needs that are currently unmet by milk banks. Our data support this perspective.

Most parents were seeking milk for an infant who is healthy and full-term:
- 83% of recipient infants were born >37 weeks gestation and healthy
- Average age of recipient infants was 7 months
- 4% (8/206) of recipient parents reported their baby had a serious or chronic medical condition
Milk sharing is one way that families who wish to feed their baby with human milk may do so without having to navigate various institutional, geographic, economic, cultural, and medical barriers. We are learning that many parents are interested in using banked donor human milk, but are not eligible. Finding ways to expand access to banked donor milk is worthy of being a national public health priority.

MYTH 4: PARENTS ARE BLINDLY ACCEPTING MILK FROM DONORS
The idea that milk sharing is casual leads to the misconception that parents seeking milk don’t realize that there are risks, and so they fail to take any precautions to make milk sharing safer.
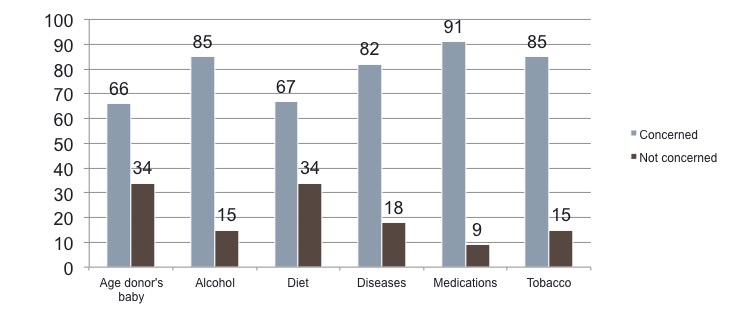
We asked recipient parents to indicate how concerned they were with milk sharing risks. Here’s what they reported:
We also asked about lay screening behaviors, defined as asking donors and recipients questions needed to make an informed decision about giving or accepting milk.

- 91% of recipients reported asking donors screening questions
- screening practices vary with different kinds of social relationships
- the higher the concern, the more likely recipients would ask a donor questions
- perceptions of risk were typically lower when a donor is a family member, friends, or local community members
We looked at screening of donors by various types of concerns that parents have about milk sharing:
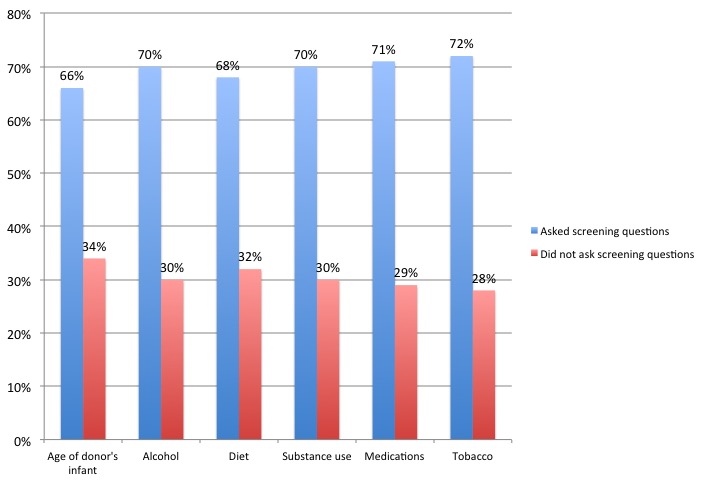
Most recipients reported gathering information about age of donor’s baby, alcohol use, diet, substance use, medication, and tobacco use. Lower rates of screening were reported when donors were family, friends, or local community members.
We also looked at screening practices for diseases, using the three most common ways parents have reported screening milk sharing donors:
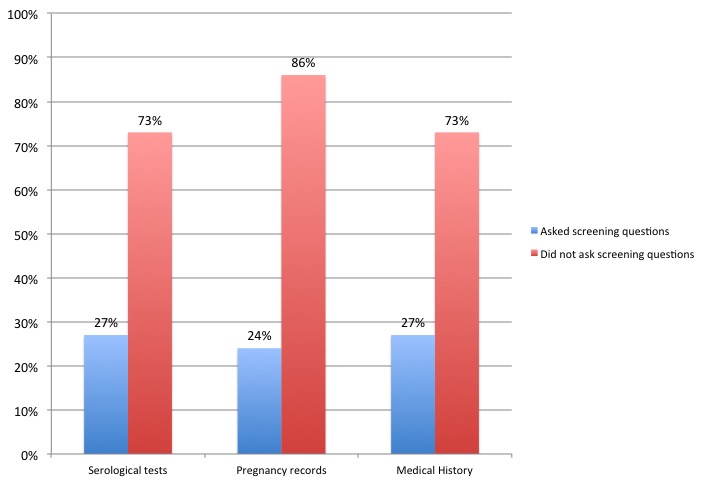
78% of recipients gathered information about disease risk in a variety of ways, including blood tests, reviewing pregnancy records, and asking questions about medical history. Screening was higher for strangers and when recipients had a high concern about disease risk.
If those numbers seem low, remember that 29% of respondents reported milk sharing with only family members or friends. So, this chart may not reflect information that recipients gather through informal conversations about risk factors and spending time with donors :
“I have only donated to close friends who already know the above information, and therefore did not need to ask.” (Donor quote)
“The one person from whom I have accepted milk was a friend whom I knew about her history, health and lifestyle that I was not compelled to ask any questions like this.” (Recipient quote)
Recipient parents also reported that donors offered information regarding their medical history, medications, substance use, and diet so that recipients would not have to ask:
“I offer these details before they are able to ask in addition to my blood test results.” (Donor quote)
“The health information is always volunteered – I don’t need to ask.” (Recipient quote)
Perceptions of risk and donor screening are highly contextual and relationship-specific. Discussing health information can sometimes be awkward, regardless if you know someone well or not. Understanding how people share health information is really important in trying to identify potential barriers to open communication about milk sharing risks.
MYTH 5: SHARING MILK IS DIRTY & DANGEROUS
So, now we get down to the big and scary clickbait headlines that talk about “the dangers of milk sharing” and milk sharing being the same as “playing Russian Roulette with your baby.” Fear tactics used in media coverage of milk sharing perpetuate the notion that breastmilk is dirty and formula, by comparison, is “clean and safe.”

There are relative risks, benefits, and costs associated with any type of infant feeding option. The key public health risks of milk sharing are bacterial contamination through handling practices, contamination with maternal medications and substances, and disease transmission.
The Academy of Breastfeeding Medicine has a protocol to guide safe expression, storage, and feeding practices, which minimize risk of contamination. Most breastfeeding mothers in the U.S. reported following these guidelines, at least the ones for expression and storage. Following good hygiene when expressing and storing milk is important to reducing risks of bacterial contamination.
If milk thaws during transit, there is a possibility that it could lead to a proliferation of harmful bacteria, which might spoil the milk. When human milk is shipped between milk sharing families, there is careful coordination between donors and recipients regarding how to package and ship the milk to avoid thawing and spoiling. But, most milk sharing occurs locally with in-person, face-to-face drop offs and pick ups – this helps to keep the milk frozen en route. Not to mention that 12% of donors in our study reported breastfeeding a recipient baby. A milk sharing study in Central Florida found similar results.
We know from the scientific literature that expressed human milk is resistant to bacterial contamination under a variety of expression, freeze-thaw, and handling conditions. Freshly expressed breastmilk can be fed to a healthy baby after sitting at room temperature for around 8 hours, used after being refrigerated for about a week, and previously frozen milk is considered good within about 24 hours after thawing for feedings.

The definition of bacterial “contamination” is somewhat contentious (hence the scare quotes), as human milk naturally contains beneficial bacteria. Infants are exposed to bacteria in the womb, during birth, through contact with normal flora of a caregiver’s skin, and in their everyday environments. The bacteria found in milk are essential to the development of a healthy neonatal gut microbiome and immune system. More to the point, we do not have a robust evidence-base to determine what levels of bacterial growth lead to adverse health outcomes in healthy, immunocompetent infants.
A study of milk bought anonymously online found evidence of tampering with cow’s milk, presumably to increase the seller’s profit, as milk is usually paid for by the ounce. Unlike with milk sales, there is no financial incentive for milk sharing donors to increase the volume of milk that they share. We don’t yet have evidence for milk bank donations or milk sharing, but tampering with milk in this way is not considered a risk for altruistic donations.

Some have claimed that milk sharing is also dangerous because donors are not going to disclose their use of illicit drugs, alcohol, nicotine, or medications they take. It is true that milk sharing relies on relationships of trust. We see from our study that milk sharing recipients gather information for things they are concerned about.
In terms of the risks of exposures to medications and substances in milk, it’s helpful to understand what the recommendations are for mothers who are breastfeeding their own healthy, full-term babies. Most medications are considered safe while breastfeeding, and neither smoking nor consuming caffeine or alcohol are considered reasons not to breastfeed.
But, what about the DISEASES!! It is important to remember that the available evidence shows that the risks of diseases that may be passed via human milk are relatively low. This is one reason that there are so few diseases that are considered incompatible with breastfeeding. It is also why milk sharing between a healthy donor and a healthy infant is supported by WHO-UNICEF when mother’s own milk is not available.
HIV/AIDS is arguably the disease that causes the most concern, because of how complex transmission is. There are several reasons why the risk of HIV transmission through informed milk sharing are thought to be relatively low in the U.S.
- Mothers in the U.S. are tested for HIV during pregnancy to reduce rates of perinatal transmission and are discouraged from breastfeeding.
- The CDC notes that the risk of transmission from a single bottle of expressed milk is low, and that freezing may even attenuate the risk of transmission.
- The rates of HIV transmission via seroconversion during lactation in the general U.S. population are not so high as to mandate that all mothers have routine HIV testing during the time in which they are breastfeeding.
Does this mean that U.S. parents shouldn’t care about HIV while milk sharing? Of course not!
- Knowing a donor’s HIV status is important. Being familiar with the risk factors of HIV transmission is important. Routine HIV testing throughout the time donors are sharing their milk is one way to further reduce potential risk of HIV transmission to a recipient baby. If for nothing else, it provides peace of mind. We see this happening regularly in practice.
- Healthcare facilitated milk sharing is another model of practice that may reduce the risks of HIV and other forms of contamination. Organizations like Mothers’ Milk Alliance and Get Pumped! support this type of milk sharing. They provide serological testing, instructions for how to express, store, and handle the milk, breastfeeding support, and they coordinate the distribution of milk to recipients.
- HIV is killed through flash heating milk, a simple practice that can completely eliminate the risk of transmission. Around 10% of recipients reported flash heating milk, and these were recipients who were highly concerned with disease transmission.
Key Takeaways
Milk sharing is nested within complex social relationships. While laboratory tests of milk are essential to understanding relative risks and benefits, milk sharing research needs social scientists to shed light on contextual factors that shape infant feeding decisions and practices.

The more we learn about milk sharing practices, the better we are able to:
- support parents and other caregivers to make informed infant feeding decisions
- discuss the evidence-based risks, benefits, and costs of milk sharing in ways that are not stigmatizing or fear-based
- understand the circumstances in which parents accept or refuse milk
- understand the circumstances in which donors share their milk
- design studies to assess milk sharing risks that reflect what people are doing
You can read our paper here (Hooray Open Access)!

Great busting of myths with cool sciencey research. But this also articulates how fundamentally, breast milk is a very highly valued substance.
LikeLiked by 1 person
Dear Aunchalee Palmquist,
Could You give your permission for translation and publish this article on our website http://milkmama.info?
“Milk Mama” – a community helping mothers in free milksharing in Russia.
We will state You as the author, of course, and put a link to your website.
Thank You very much in advance
Regards,
Olga
LikeLike
Yes, I am very pleased to do this!
LikeLike